Maternal suicide is a leading cause of maternal mortality in the United States, accounting for roughly 20% of postpartum deaths. When a person (including those who are pregnant or postpartum) experiences a severe mental health crisis, providers and families often default to sending her to the emergency room (ER).
However, emerging research and clinical consensus show that standard ERs are frequently ineffective and can even be counterproductive for suicide care.
Standard emergency room protocols and ER staff training usually focus on short-term physical safety rather than addressing underlying psychiatric issues.
The Reality of ER-Based Care for Perinatal Crises
Emergency departments are designed to triage, stabilize, and discharge patients with physical trauma. They are structurally poorly suited to handle the nuanced, highly sensitive nature of maternal psychiatric emergencies.
Overstimulating and Traumatizing Environments
Studies confirm that psychiatric patients often view the traditional ER environment as traumatizing and invalidating. Triage relies on checking boxes rather than therapeutic engagement, which fails to predict or mitigate post-discharge risk. The majority of emergency medicine residency programs lack specialized training in psychiatric emergencies or perinatal mental health. For a person who is pregnant or in the postpartum period already dealing with sleep deprivation, hormonal fluctuations, or postpartum psychosis, the stimulation in an ER and lack of validating support can exacerbate symptoms.
ER “Boarding” Times
Patients experiencing mental health crises routinely face long “boarding” periods, frequently waiting 18 hours or more in the ER before seeing a specialist. For a postpartum mom, these extensive delays present specific complications:
- Prolonged separation from her newborn, disrupting critical bonding periods.
- Inadequate accommodations or equipment for breast pumping, risking physical complications like mastitis.
- Intensified feelings of isolation, fear, and abandonment while waiting.
Discharged to No Care – Back to Square One
ER doctors and nurses are often rushed, generally operate in silos, and rarely coordinate directly with a patient’s OB/GYN, midwife, or any existing mental health provider. So while a referring provider may feel sending a patient who marks “yes” to thoughts of harming oneself on a screener is the best way to help the patient, the reality is the patient will be discharged with no plan of care and likely no connection to psychiatric help.
Heightened Post-Discharge Risks
Data from a landmark JAMA Psychiatry study found that individuals discharged from an emergency department following suicidal ideation or self-harm face a significantly elevated risk of suicide in the immediate year post-discharge. Temporary stabilization without integrated, specialized perinatal follow-up fails to resolve long-term risk.
Building a Safer, Maternal-Centered Crisis System
Addressing this gap requires moving away from emergency rooms as the default solution and building specialized crisis pathways.
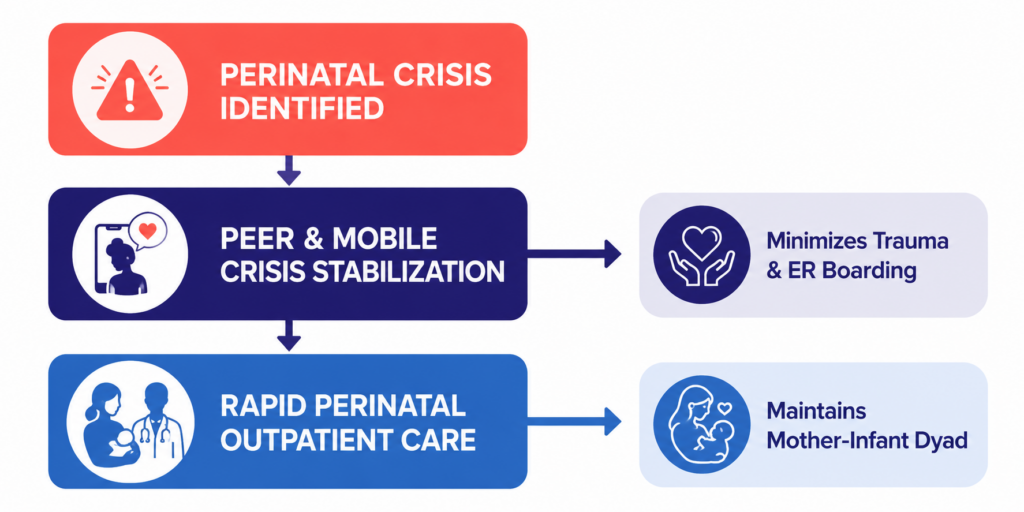
- Utilize dedicated crisis lines: Providers and families should leverage specialized resources like the 988 Suicide & Crisis Lifeline for immediate, non-hospital support.
- Invest in mobile crisis teams: Mobile units can meet a mother in her home (or at the OB clinic), stabilizing her in a familiar environment without enforcing a disruptive hospital stay.
- Expand perinatal psychiatry access: Health systems must implement coordinated referral networks that route high-risk mothers directly to outpatient reproductive psychiatrists and/or residential treatment or intensive outpatient programs (IOPs)/partial hospitalization programs (PHPs) within 24 to 48 hours.
The Policy Center continues to advocate for policy changes, including federal guidelines like the CMS hospital readiness updates that mandate better preparation for obstetric and perinatal mental health emergencies. True maternal health equity requires a system that delivers specialized, compassionate care to mothers exactly when they need it most.