Introduction
Maternal suicide is a leading cause of maternal mortality in the US.1 While maternal mortality has rightfully garnered increasing attention in recent years, maternal suicide has been historically overlooked as a cause of maternal mortality because national maternal mortality rates previously excluded suicides as pregnancy-related deaths, instead classifying maternal suicides deaths as incidental or accidental deaths.2

According to the Centers for Disease Control & Prevention (CDC), there was a record high number of deaths in 2022 from suicide for the general US population. It is important to continue to address suicide prevention efforts for the general and maternal population.3
In 2024, the Task Force on Maternal Mental Health recognized maternal mortality as a priority issue in the US.4 As national and state efforts to address maternal mortality through improved public health data collection have increased, maternal suicide has emerged as one of the top three causes of pregnancy-associated deaths, highlighting the need to address maternal suicide as a contributing factor of maternal mortality in the US.5 It is estimated that up to 20% of perinatal maternal deaths are due to suicide,5 making maternal suicide deaths more common than deaths caused by postpartum hemorrhage or hypertensive disorders.6
While challenges to standardize and improve public health data collection from state to state still exist, state Maternal Mortality Review Committees (MMRCs) are increasing consistency regarding how they review and document maternal deaths.
The Centers for Disease Control (CDC) has determined, using the data from 36 state MMRCs, that mental health conditions are a leading underlying cause of pregnancy-related death.7
Maternal Mental Health Conditions are defined by the CDC as “suicide, overdose/poisoning related to substance use disorder, and other deaths determined by the MMRC to be related to a mental health condition, including substance use disorder” Maternal Mental Health Conditions account for almost 23% of pregnancy-related deaths and 80% of pregnancy-related deaths are determined to be preventable.7
As maternal suicides have a lasting and far-reaching societal impact, it is important to prioritize maternal suicide prevention efforts. The negative impact of maternal mental distress and illness on child development is well-documented, as well as the impact of maternal suicidality on child wellness. Additionally, women diagnosed with postpartum depression have an elevated risk for suicide up to 18 years postpartum,8 showing the vast impact maternal depression and suicidality can have across a woman’s lifespan. Thus, it is important to further examine how to prevent maternal suicides through clinical, systems, and policy shifts.
Understanding Maternal Mortality Definitions

“Pregnancy-Associated” Death: According to the CDC, death during or within one year of pregnancy, regardless of the cause. These deaths make up the universe of maternal mortality; within that universe are (1) pregnancy-related deaths and (2) pregnancy-associated, but not related deaths.9
One way to differentiate between Pregnancy-RELATED and
Pregnancy Associated, but NOT RELATED death is to ask the question:
“Would the woman have died if she wasn’t pregnant?”
✗ If the answer is no , then it is a pregnancy-related death .
✗ If the answer is yes , then it is a pregnancy-associated, but not related, death.10
Risk Factors and Correlations
As the causes of maternal suicide are complex and multifaceted, an understanding of the spectrum of maternal suicide risk factors is necessary to formulate and adopt appropriate preventive and treatment measures.
Behavioral Health Risk Factors
The most potent risk factors are personal and/or family history of psychiatric disorders, a prior suicide attempt, or suicidal ideation.5 Increased symptoms of anxiety have been linked to frequent thoughts of self-harm in depressed postpartum women.11 A bipolar disorder diagnosis puts a woman at increased risk for postpartum psychosis, thus also increasing their risk for maternal suicide.12 According to the CDC, 34% of pregnancy-related suicides had a documented prior suicide attempt.13 Women with a postpartum psychiatric admission were 70 times more at risk of suicide in their first postpartum year.14 Studies on the general population have shown that 45% of those who die by suicide see their primary care physician within a month of their death.15 Eighty-four percent of those who die by suicide have had a health care visit in the year before their death. 16 Almost 40% of individuals who died by suicide had been to the emergency room, but did not have a prior mental health diagnosis.17 In general, the perinatal and postpartum population has significantly more contact with healthcare providers, increasing touchpoints for screening and referral to appropriate treatment.
This data continues to reinforce the importance of universal screening for all maternal mental health disorders, as well as continuing support and care for women in the postpartum period as an initial step to preventing maternal suicides.
Environmental and Social Risk Factors
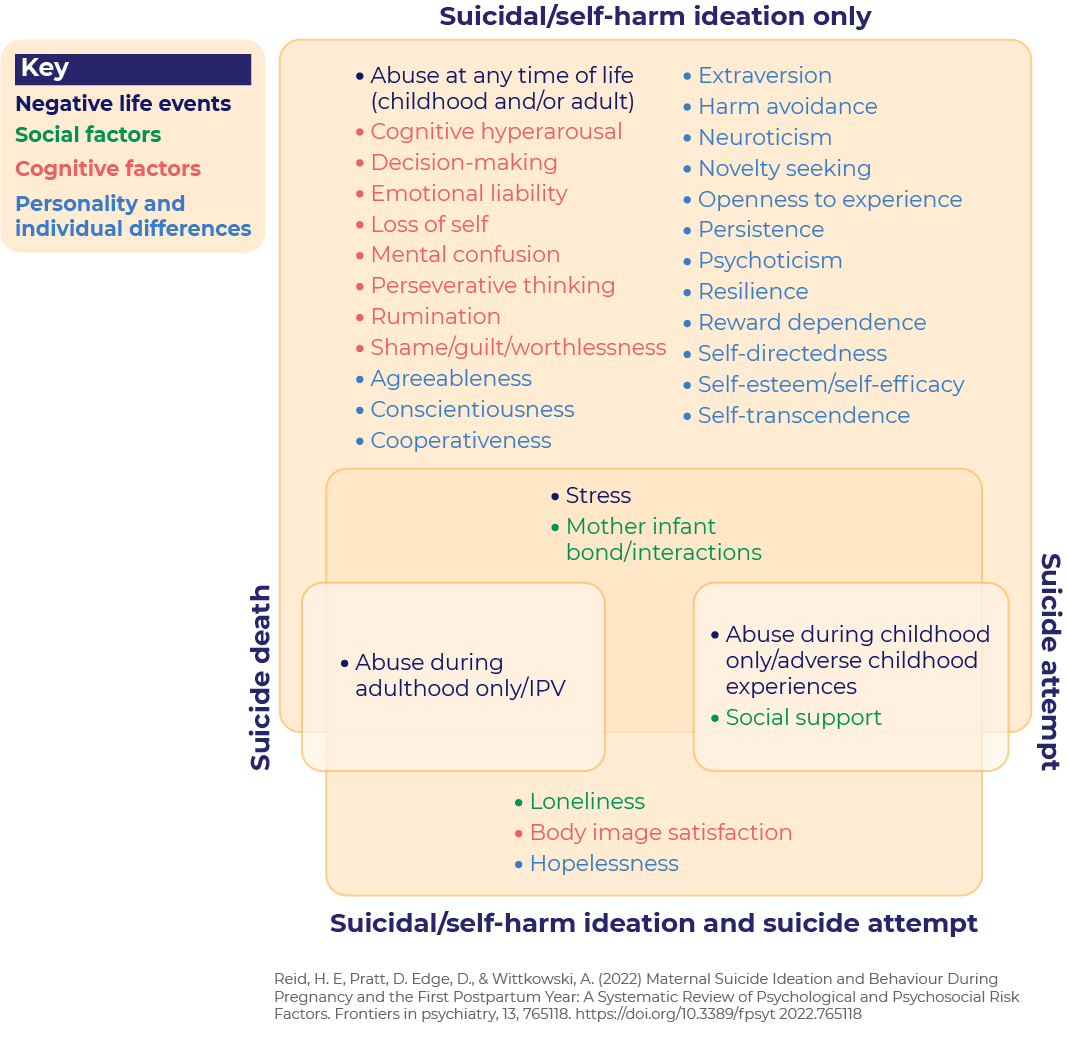
There is also strong evidence that abuse experienced at any time in a woman’s life increases the risk of suicidality (suicidal ideation, attempted suicide, death from suicide) during pregnancy and the first postpartum year. Women experiencing suicidality are more likely to experience intimate partner problems, depressed mood, substance abuse, physical health problems, and have experienced recent bereavement.18 Lack of social support during the perinatal period is also strongly associated with suicidal behavior.19 Further, sleep disturbances significantly increase the likelihood of suicide attempts and suicidal thoughts in adults20 and increase thoughts of self-harm in depressed postpartum moms.21
Other risk factors for maternal suicide and/or suicidal ideation include: young age, family conflict, loneliness, and unwanted or unplanned pregnancy.1 Environmental risk factors such as exposure to disaster, conflict, or war, social and gender inequalities, racial discrimination, belonging to an ethnic or religious minority, having crowded or inadequate housing, and living in rural areas can also elevate the risk for maternal suicide.1
Timing of Maternal Suicides
Research shows that certain times during the perinatal and postpartum periods have elevated risks for maternal suicide. While maternal suicides can happen during pregnancy, most maternal suicides occur in the postpartum period–and not just in the immediate postpartum period. In fact, 62% of pregnancy-related suicides occur between 43-365 days postpartum, followed by 24% during pregnancy and 14% within 42 days postpartum.12 Another study conducted in California yielded a similar result, showing that maternal suicides are most frequently completed between 6-12 months (151-365 days) postpartum.22
The data on risk factors, timing of maternal suicides, and frequency of provider contact prior to a suicide/suicide attempt reveals critical periods and areas for suicide prevention techniques, mental health and suicide risk screening, and other social and behavioral interventions that can help lower maternal suicide risk. The data further shows that signs of maternal suicides exist, and this data should be utilized in future research to develop effective interventions for preventing maternal suicides.
What is Suicidal Ideation?
Suicidal ideation (SI), also known as having suicidal thoughts, is a broad term used to describe a range of ideas, ruminations, and general contemplations about suicide. Broadly defined, suicidal ideations exist on a spectrum, ranging from passive suicidal ideations (a wish to die with no intent/plan on inflicting self-harm) to active suicidal ideations (a current active desire to inflect self-harm that results in death).
It should be noted there currently is no standardized definition for suicidal ideation.23 However, the Columbia–Suicide Severity Rating Scale (C-SSRS), is a validated assessment tool that evaluates suicidal ideation and behavior that has been adopted and endorsed by the Food and Drug Administration (FDA), the Center for Disease Control (CDC), World Health Organization (WHO), and many other health agencies as the standard for evaluation suicidal ideations.24 The C-SSRS delineates five subtypes of suicidal ideation (wish to be dead, nonspecific active suicidal thoughts, suicidal thoughts with methods, suicidal intent, suicidal intent with plan25) along with five subtypes of suicidal behavior (actual attempt, aborted and interrupted attempts; preparatory behavior; suicide), and self-injurious behavior without suicidal intent.26 The C-SSRS should be used when assessing someone with suicidal ideations.
Race and Maternal Suicide
Recent research reveals that American Indians and Alaska Natives have much higher rates of pregnancy-associated drug-related death and suicide compared with all other racial or ethnic groups. The 2022 Pregnancy-Related Deaths Among American Indian or Alaska Native Persons: Data from Maternal Mortality Review Committees in 36 US States, 2017–2019 report from the CDC showed that mental health conditions are the top underlying causes of pregnancy-related death among American Indian or Alaska Native persons, accounting for 31.3% of deaths with a known underlying cause.27 The Suicide Prevention Resource Center’s (SPRC) annual Tribal Suicide Prevention Needs Assessment (TNA) examines the suicide prevention infrastructure and capacity of U.S. Tribes and Tribal health boards. Findings from the most recent report identify resources for Tribal suicide prevention and should be reviewed for potential integration opportunities into tribal maternal healthcare systems.28
Non-Hispanic White people have the second highest rates of pregnancy-associated drug and suicide death. Non-Hispanic Asian and Pacific Islander people, who have the lowest pregnancy-associated death ratio for both drug-related deaths and homicide, have the third highest ratio for suicide. Pregnancy-associated drug-related deaths are most common among those aged 35 years or older, whereas suicide and homicide were most common among the youngest birthing people.29
BIPOC and Suicidal Ideations
Studies show that Black, Indigenous, and People of Color (BIPOC) women have a higher risk for suicidal ideations, while non-Hispanic White women have a higher risk of suicide. Women who self-report as “other race” are almost 3 times more likely than white women to report suicidal ideation in the postpartum period.30 In the immediate postpartum period, Asian women are 9 times more likely to report suicidal ideation than their white counterparts. Hispanic and Black women are 2 times more likely to report suicidal ideation than white women.29
Suicide Prevention and Treatment
Screening for Maternal Suicide Risk
Screening has been a recent focal point in maternal mental health.31 In the last decade, most government entities and professional associations such as The American Academy of Pediatricians (AAP),32 The American College of Obstetrics and Gynecology (ACOG),33 The U.S. Preventive Services Task Force (USPSTF),34 The Centers for Medicare and Medicaid Services (CMS)35 and others have prioritized and endorsed screening for maternal mental health disorders, mainly maternal depression, and anxiety.

In February 2023, the Alliance for Innovation on Maternal Health (AIM) issued a safety bundle addressing perinatal mental health. AIM defines patient safety bundles (PSB) as “…collections of evidence-informed best practices, developed by multidisciplinary experts, which address clinically specific conditions in pregnant and postpartum people…[and] includes actionable steps that can be adapted to a variety of facilities and resource levels.”36
The bundle addressed screening maternal suicide stating that when “…concern exists for suicidality due to response in depression screening tool or interaction with patient, further assessment is required. This is done with a clinical interview and can include a suicidality specific screening instrument.”35
In June 2023, The USPSTF issued a recommendation on depression and suicide screening. While screening for depression was recommended for all adults, including pregnant and postpartum persons, the task force concluded that “the current evidence is insufficient to assess the balance of benefits and harms of screening for suicide risk in the adult population, including pregnant and postpartum persons.” 37
The most commonly used screeners for maternal depression and anxiety are: the Patient Health Questionnaire (PHQ 2 or 9), the Generalized Anxiety Disorder screener (GAD 3 or 7), and Edinburgh Pregnancy/Postnatal Depression Scale (EPDS).30
There is a single question on both the PHQ-9 and EPDS screening tools asking if a person has had suicidal thoughts. While this is a good first step to screening for suicide risk, having suicidal thoughts does not necessarily mean someone is acutely suicidal or at immediate risk of imminent harm.
Screening for Suicide Risk – A Critical Step to “Do No Harm”
If a person answers yes to having had suicidal thoughts, then the Columbia-Suicide Severity Rating Scale (C-SSRS) and Suicide Assessment Five-Step Evaluation and Triage (SAFE-T) screeners or the Ask Suicide-Screening Questions (ASQ) Tool should be used to assess for suicide risk. 38,39 The Patient Safety Screener (PSS), is another screening tool used for identifying patients in the acute care setting who may be at risk of suicide. The PSS-3 can be administered to all patients who come to the acute care setting, not just those presenting with psychiatric issues.40 All of these are prominent evidence-based suicide screening and risk assessment tools that should be used in the perinatal and postpartum period by front-line providers like Ob/Gyns.
It is important to note that screening for suicide risk is only one part of the process used to identify suicide risk. There should also be a process in place for further assessment and risk formulation.41
If a person is identified as being at risk for suicide, a clinical workflow needs to be followed that all staff are trained in that emphasizes reducing access to lethal means, developing a collaborative safety plan, initiating treatment that targets suicidal thoughts and behaviors directly, and providing caring contacts that include warm hand-offs to skilled providers.42 Providers are encouraged to look at Zero Suicide to learn more about effective suicide care.
Self-Harm
Though a suicide attempt is considered self-harm, not all forms of self-harm indicate a potential suicide attempt. For example, a person may engage in cutting to relieve distress and may not be suicidal.43 The current data on nonsuicidal self-injury (NSSI) and suicide risk indicated that certain specific NSSI characteristics such as type, frequency, effectiveness,44 and age may increase suicide risk.45 However, more research is needed to better understand any correlation between NSSI and suicide risk. This is why it is important to use a screening tool like the C-SSRS to screen for potential suicide risk should a mother describe a history of self-harm. Since NSSI may also be associated with obsessive-compulsive disorder,46 a clinician may also want to screen for OCD.
Do Intrusive Thoughts About Suicide Increase Risk?
Experiencing “intrusive” or unwanted thoughts is common during the perinatal period. Research has shown that 70-100% of new moms experience unwanted thoughts about infant-related harm, and as many as 50% report unwanted thoughts about harming their infants on purpose. However, research also shows that these intrusive thoughts, while distressing, do not actually increase the risk of infant-harming behavior.47
Currently, there is a lack of research on whether intrusive thoughts about suicide increase the risk of suicide. If a mom has thoughts about self-harm, it is important to screen her for suicide risk to further evaluate whether the thoughts are intrusive thoughts about suicide or suicidal ideations. If the clinician suspects intrusive thoughts related to OCD or if the thoughts are described as unwanted or intrusive, it is also important to screen the patient for OCD. The OCI-12 is a great tool to identify intrusive thoughts and further differentiate them from suicidal ideations.48
Treatment
Evidence-based Interventions

Historically, clinicians have sought to treat patients with suicidal behavior and thoughts by solely treating their mental health problems (such as depression, anxiety, and substance use disorder).49 Recent research shows that effective treatment for suicide risk must target suicidal ideation and behaviors specifically, through evidence-based models of treatment designed specifically to reduce suicidal behavior/attempts. If other mental health issues are presented, treatment for these mental health issues should also be administered, not as a treatment for suicide, but as a concurrent treatment.50
Evidence-based intervention and treatment for suicide risk are designed to specifically target suicide risk. These following interventions have been proven to be effective in reducing suicidal thoughts and behaviors:
- Cognitive Behavioral Therapy for Suicide Prevention (CBT-SP)
- CBT-SP is grounded in principles of CBT and targeted therapies for suicidal and depressed patients.51
- It includes cognitive restructuring, emotion regulation, and problem-solving strategies as well as behavioral activation.50
- Studies show that CBT-SP reduces suicide attempts and symptoms in adults and adolescents.52,53
- Dialectical Behavioral Therapy (DBT)
- DBT is based on CBT and has four components: a skills training group meeting once a week for 24 weeks, individual treatment once a week, running concurrently with the skills group, phone coaching, upon request by the client, consultation team meetings—a kind of “therapy for the therapists”54
- Numerous research studies, including several randomized control trials55, have shown DBT to be effective in reducing suicidal behavior and other behavioral health issues.50
- Those receiving DBT are significantly less likely to: drop out of treatment, attempt suicide, visit psychiatric emergency rooms, experience psychiatric hospitalization.54
- Collaborative Assessment and Management of Suicidality (CAMS)
- CAMS is an intensive psychological treatment that is suicide-specific, helping patients develop other means of coping and problem-solving to replace or eliminate thoughts of suicide as a coping strategy.50
- CAMS is designed for outpatient care settings and has been used successfully in outpatient and inpatient settings, as well as with college students and military personnel.
- CAMS has been validated as an evidence-based intervention for the past 30 years. Using CAMS has:
Least Restrictive Care

Recent research has suggested that treatment should be carried out in the least restrictive setting possible for the patient.61 It is important for the clinician to be adequately trained to develop an outpatient intervention, with an abundance of appropriate support, and avoid hospitalization if possible.50
Currently, the recommended model of care for suicide prevention is called the Stepped Care Model, where patients are “offered numerous opportunities to access and engage in effective treatment, including standard in-person options as well as telephonic, interactive video, web-based, and smartphone interventions.”60 While the levels may vary, the following are the main groups that make up the care model, from least restrictive to most restrictive:
- Crisis Care and Support
- Brief Intervention
- Suicide-specific outpatient (addressed earlier in the section: Evidenced-Based Interventions)
- Emergency Respite Care
- Partial hospitalization, with suicide-specific treatment
- Inpatient psychiatric hospitalization, with suicide-specific treatment
It should also be noted that the least restrictive care model means that treatments tend to also be more accessible and cost-efficient. It should be noted that concerns regarding access to child care and caretaking responsibilities are a major barrier to suicide care for the perinatal and postpartum population. Thus, the least restrictive care model may offer more reasonable and accessible methods of treatment for moms.
Crisis Care and Support
Currently, the gold standard for suicide crisis care in health delivery systems includes:50
- mobile crisis teams
- walk-in crisis clinics, including mental health urgent care centers
- hospital-based psychiatric emergency services
- peer-based crisis services
- any other programs designed to provide assessment, crisis stabilization, and referral to an appropriate level of ongoing care.
Crisis care and support services are especially helpful to patients with barriers to accessing mental healthcare. It is important for these services to have basic familiarity with maternal mental health disorders so that they can provide better care coordination and support for the perinatal and postpartum population in crisis situations.
Brief intervention and follow-up

Brief interventions are focused on helping the patient increase awareness and insight regarding their behavior and motivate them towards behavioral change.62 Widely used in substance abuse prevention, generalizing the use of brief interventions into suicide prevention has shown promising outcomes.50
The Stanley-Brown Safety Plan is a validated brief intervention that is widely used by clinicians to collaboratively mitigate acute suicide risk with a suicidal individual.63 The intervention can be used in most environments and can be adapted for specific populations,64 such as women in the perinatal and postpartum period.
Emergency respite care
As psychiatric hospitalizations are increasingly being recognized by the suicide prevention community as an intervention of last resort, respite centers that are usually located in residential facilities are an alternative to hospitalization. Research shows that individuals in crisis may prefer a respite care setting to hospitalization.65
Respite centers may also employ peer support specialists as staff. Recent pilots training peer support specialists specializing in maternal mental health have garnered a lot of interest and support for the use of peers with lived experience to support the perinatal and postpartum population.66 Research shows that respite care may yield better outcomes than acute psychiatric hospitalization.50
Partial hospitalization, with suicide-specific treatment
Partial hospitalization provides a structured program of outpatient psychiatric services as an alternative to inpatient psychiatric care. The patient receives
intensive treatment during the day, but does not need to stay overnight.67 There are currently 31 intensive outpatient and partial hospitalization perinatal psychiatry programs spread out over 17 US states and Washington, DC.68
Inpatient psychiatric hospitalization, with suicide-specific treatment
Inpatient hospitalization is the most restrictive and expensive treatment for suicide risk.50 Most inpatient patients do not receive suicide-specific treatment aimed at reducing suicide attempts and risk after they are discharged.69 Some research shows that patients may actually be at higher suicide risk in the immediate period after being discharged from hospitalization.70
To date, there are only 3 inpatient perinatal psychiatry programs in the US: UNC Perinatal Psych Inpatient Unit, Northwell Health Perinatal Psychiatry Service, and El Camino Inpatient Psychiatric Care Women’s Specialty Unit. The lack of specialty perinatal psychiatry programs in the US presents yet another barrier to care for the perinatal and postpartum population.67
The Zero Suicide Framework
As suicide is a complex problem, effective suicide prevention requires a range of interdisciplinary strategies, policies, and interventions. In 2012, the U.S. Surgeon General and the National Action Alliance for Suicide Prevention issued a National Strategy for Suicide Prevention.71 In this strategy report, a concept known as Zero Suicide was identified as a framework for systemwide transformation towards safer suicide care within the healthcare system.37 Today, Zero Suicide is considered the gold standard for suicide care in the US health care system.72 Recent research has shown that implementation of Zero Suicide has reduced suicide in patients.73
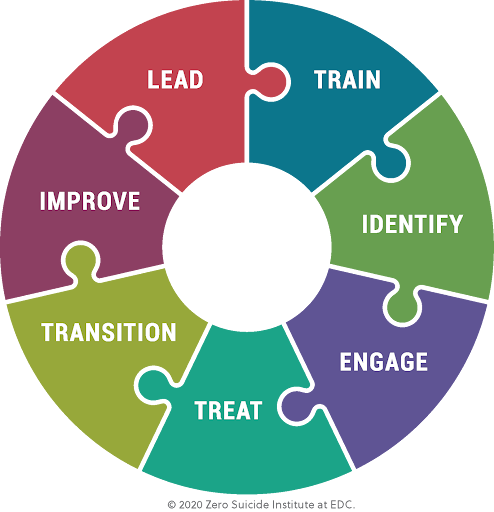
Zero Suicide Model
The Zero Suicide Model is made up of seven elements: lead, train, identify, engage, treat, transition, and improve. These elements are the core components of safe care for individuals with suicidal thoughts and urges. It is the use of these elements as a bundle that effects change and makes up a holistic approach to suicide prevention within health and behavioral health care systems.37 The Zero Suicide Toolkit is a resource that describes each element in detail.
As maternal suicide has only begun to garner much-needed attention the last few years, research specific to maternal suicide prevention strategies has been scarce. Since the Zero Suicide model has been effective across many populations, the adoption of the model and practices into the maternal healthcare system would be a step in the right direction towards preventing maternal suicide.
National Strategy for Suicide Prevention
In 2024, a new National Strategy and National Federal Plan for Suicide Prevention was released by the Federal government. The National Strategy presented a 10-year plan that provides comprehensive recommendations addressing gaps in the suicide prevention field. The four main strategic direction of the strategy are:
- Community-Based Suicide Prevention
- Treatment and Crisis Services
- Surveillance, Quality Improvement, and Research
- Health Equity in Suicide Prevention
The Federal Action Plan identifies more than 200 actions across the government to be taken over the next three years in support of these goals. These actions include:
- Evaluating promising community-based suicide prevention strategies
- Identifying ways to address substance use/overdose and suicide risk together in the clinical setting
- Funding a mobile crisis locator for use by 988 crisis centers
- Increasing support for survivors of suicide loss and others whose lives have been impacted by suicide
These actions will be monitored and evaluated regularly to determine progress and success, and to further identify barriers to suicide prevention.
These strategic goals can also provide a framework for the adoption and integration of suicide prevention strategies and policy recommendations within the maternal healthcare system.74
Data Collection on Maternal Suicide in the United States
Developing a process and method for data collection on maternal suicides has only recently begun in many states. Collecting national data on maternal suicide has been a challenge over the years due to the lack of standardization in measurement,methodology, and definition.75 The US currently does not require states to report maternal suicide rates.76 In addition, the state-based healthcare infrastructure has caused additional challenges as data collection benchmarks and definitions vary from state to state, and death by suicide may not be reviewed or reported in some states. If a state does review and report data on maternal suicide, the state may not utilize standardized criteria for independently reviewing and categorizing maternal suicide data.77
Overview of US Maternal Mortality Data Collection Methods
Maternal Mortality Review Committees (MMRCs)

In an effort to standardize the definitions, methodology, and measurement of maternal mortality in the US, the Preventing Maternal Deaths Act was passed in 2018 to fund and support state Maternal Mortality Review Committees (MMRCs).74
This funding comes from the Centers for Disease Control (CDC) and supports state agencies and organizations that coordinate and manage MMRCs to identify, review, and characterize pregnancy-associated deaths; and identify prevention opportunities.
These committees are formed at the state and sometimes at the city levels and are multidisciplinary. They include representatives from public health, obstetrics and gynecology, maternal-fetal medicine, nursing, midwifery, forensic pathology, mental and behavioral health, patient advocacy groups, and community-based organizations.
Each committee performs a comprehensive review of maternal deaths during pregnancy and within a year of the end of a pregnancy. Among pregnancy-related deaths with an MMRC-determined manner of death, 8.4% were determined to be a suicide.7
MMRCs and the Enhancing Reviews and Surveillance to Eliminate Maternal Mortality (ERASE MM) Program
As of 2024, the CDC has funded 46 states and 6 US territories and freely associated states to be a part of the “Enhancing Reviews and Surveillance to Eliminate Maternal Mortality” (ERASE MM) program, which provides guidelines and technical assistance to MMRCs in reviewing pregnancy-associated deaths to improve consistency of the data collected through the CDC’s Maternal Mortality Review Information Application (MMRIA). Jurisdictions funded through the ERASE MM Program are required to use MMRIA for abstracting data and entering committee decisions.78,79 This data can better inform recommendations for preventing future deaths.
There has also been an effort on behalf of the CDC to increase accuracy in determining whether a death was a suicide versus an overdose, through MMRC’s use of key informant interviews. These in-depth reviews, when standard guidelines are used, can provide a more accurate count of maternal suicides and determine clinical and non-medical contributors to inform public health interventions.80
Pregnancy Mortality Surveillance System (PMSS)
Prior to the increase in MMRCs due to the passage of The Preventing Maternal Deaths Act, the CDC had previously conducted national pregnancy-related mortality surveillance using only the Pregnancy Mortality Surveillance System (PMSS). This system relies on the use of death records and defines a pregnancy-related death as the death of a woman while pregnant or within one year of the end of pregnancy from any cause related to or aggravated by the pregnancy. This system uses medical epidemiologists to review and analyze death records, linked birth records and fetal death records if applicable, and additional available data from all 50 states, New York City, and Washington, D.C.
Generally, the pregnancy-relatedness cannot be determined in PMSS for injury deaths such as drug overdoses, suicides, or homicides and therefore suicide isn’t reported through the CDC’s PMSS system.
Perinatal Quality Collaboratives (PQCs)
Perinatal Quality Collaboratives (PQCs) are state or multistate networks of teams working to improve the quality of care for mothers and babies. Committee members identify healthcare processes that need to be improved and use the best available methods to make changes as quickly as possible. The CDC’s Division of Reproductive Health (DRH) is currently providing support for 36 state-based PQCs.81 Some PQCs such as Colorado’s PQC are in the early phase of evaluating effective maternal suicide prevention strategies and should have intervention plans and outcomes data to share in the coming years.
Accidental Drug-Related Death and Suicide: A call for a Standardized Review Process
Suicide and drug-overdose deaths make up the category of pregnancy-related deaths due to mental health conditions, and are two of the leading causes of maternal mortality in the US. In the most recent CDC report released in 2022 on pregnancy-related deaths from 2017-2019 reviewed by MMRCs in 36 states, mental health conditions were the most frequent underlying cause of death, accounting for 22.7% of deaths.7

A 2021 analysis of the 2008-2017 pregnancy-related mental health deaths showed that 63% of the pregnancy-related deaths with mental health conditions as the underlying cause of death were by suicide and 24% were by unintentional poisonings/overdoses.82
There currently isn’t a national standardized review process for MMRCs when evaluating whether a suicide or drug-related death should be categorized as pregnancy-related or pregnancy associated. As substance use disorders increase relative suicide risk for women83 and are intricately associated with other mental health disorders,84 it can sometimes also be a challenge for MMRC’s to delineate between a suicide via overdose and an accidental overdose without additional information from an informant interview or a standardized classification process to help MMRCs make objective and consistent assessments.
In response to these concerns and the clear need to have an evaluation process, Utah’s MMRC developed a standardized evaluation tool to assess accidental drug-related death and suicide beginning in 2015 and performed a retrospective case review of all pregnancy-associated deaths and pregnancy-related deaths evaluated by Utah’s MMRC from 2013 to 2016. This evaluation tool also categorized suicide and drug-related deaths independently. After application of standardized criteria, the Utah MMRC determined that pregnancy itself was the inciting event leading to the majority of accidental drug-related deaths or suicides among pregnant and postpartum women.76 The CDC is actively in the process of engaging all MMRCs in the country in a Delphi survey to achieve national consensus for what constitutes a pregnancy-related death from suicide or overdose.
Discussion and Recommendations
Suicide has consistently been a complex public health problem within the general US population. Between 2000-2018, suicide rates increased 37%. While suicide rates decreased 5% between 2018-2020, these rates returned to their peak in 2022.3,85 Maternal suicidality has tripled over the last decade.86 As the maternal healthcare system has only recently begun to look into the epidemiology of maternal suicide, more research is needed to better understand the intricate causes of maternal suicide and better data collection methods can help close the evidence gap and advance systems change.

As the Zero Suicide framework has been the gold standard for suicide prevention since 2012 and has shown to be effective across various healthcare settings and populations, maternal healthcare settings should adopt the Zero Suicide framework to prevent and reduce maternal suicides and payers should pay for implementation and reimburse for suicide assessment and provider care coordination and preventive interventions.
As part of the Zero Suicide model to reduce the burden on patients to talk about suicide, clinicians should be adequately trained in suicide prevention-specific strategies to initiate and follow through on discussions about suicide. Research suggests that most providers have little to no training in suicide prevention and care, and most report feeling uncomfortable and unprepared.87 As there are recent reports of a shortage of providers trained in DBT therapy for suicide prevention in adolescents, similar shortages are likely to exist for the adult and maternal populations.88 Therefore, having more maternal healthcare workers trained in suicide prevention would be beneficial. In fact, clinicians (ob/gyns, reproductive psychiatrists, maternal-fetal specialists, etc.) and non-clinicians (doulas, peer-support specialists, midwives) should receive suicide-specific training appropriate for their level of patient engagement.89
As maternal suicides often involve a violent method of death,18 it is crucial clinicians and social services providers are trained on how to counsel on reducing access to lethal means.
In addition, professional organizations and boards should develop a pathway for their members to receive suicide-specific training and be tested around core competencies.
Congress and state legislatures should adequately fund state Perinatal Quality Committees (PQCs), the bodies charged with leading maternal mortality efforts.
State PQCs should look at how they can incentivize or hold health systems accountable for the implementation of the Zero Suicide Framework, as well as the promotion of maternal mental health screening efforts in obstetric settings.
The National Committee for Quality Assurance (NCQA) should champion the development of a measure to assess for suicide screening in primary care and obstetric settings.
Conclusion
Maternal suicide is a tragedy that has rippling societal consequences as well as a lasting impact on families and communities. As public health systems shift to prioritize maternal suicide prevention efforts, research into causes and interventions for maternal suicidality must also be expanded. Efforts to nationally standardize and improve public health data collection initiatives through Maternal Mortality Review Committees (MMRCs) and Perinatal Quality Collaboratives (PQCs) must continue to be bolstered to better understand how to prevent suicides.

Maternal healthcare systems should prioritize the integration and adoption of the Zero Suicide framework, and efforts should be made to standardize suicide prevention training and screening protocols within the maternal healthcare system.
Maternal suicide is a tragedy that has rippling societal consequences as well as a lasting impact on families and communities. As public health systems shift to prioritize maternal suicide prevention efforts, research into causes and interventions for maternal suicidality must also be expanded. Efforts to nationally standardize and improve public health data collection initiatives through Maternal Mortality Review Committees (MMRCs) and Perinatal Quality Collaboratives (PQCs) must continue to be bolstered to better understand how to prevent suicides.
Maternal healthcare systems should prioritize the integration and adoption of the Zero Suicide framework, and efforts should be made to standardize suicide prevention training and screening protocols within the maternal healthcare system.
As new and emerging data continues to affirm maternal suicide as a leading cause of maternal death, the recent momentum and interest surrounding maternal suicide must be leveraged into clinical, systems, and policy shifts that propel actionable change and prevent maternal suicides.
As new and emerging data continues to affirm maternal suicide as a leading cause of maternal death, the recent momentum and interest surrounding maternal suicide must be leveraged into clinical, systems, and policy shifts that propel actionable change and prevent maternal suicides.
A special thanks to Susanna Trost, MPH, a CDC Foundation Epidemiologist placed with the Division of Reproductive Health at the Centers for Disease Control and Prevention and to Julie Goldstein Grumet, Ph.D., Director of Zero Suicide Institute at the Education Development Center, for their review and feedback on this report.
References
- Orsolini, L., Valchera, A., Vecchiotti, R., Tomasetti, C., Iasevoli, F., Fornaro, M., De Berardis, D., Perna, G., Pompili, M., & Bellantuono, C. (2016). Suicide during Perinatal Period: Epidemiology, Risk Factors, and Clinical Correlates. Frontiers in Psychiatry, 7, 138. https://doi.org/10.3389/fpsyt.2016.00138 ↩︎
- Mangla, K., Hoffman, M. C., Trumpff, C., O’Grady, S., & Monk, C. (2019). Maternal self-harm deaths: An unrecognized and preventable outcome. American Journal of Obstetrics and Gynecology, 221(4), 295–303. https://doi.org/10.1016/j.ajog.2019.02.056 ↩︎
- Centers for Disease Control and Prevention (CDC). (2024, August 5). Suicide Data and Statistics. Suicide Prevention. https://www.cdc.gov/suicide/facts/data.html ↩︎
- Office on Women’s Health. (n.d.). Task Force on Maternal Mental Health. Retrieved March 19, 2024, from https://www.womenshealth.gov/about-us/what-we-do/working-groups-and-committees/task-force-on-maternal-mental-health ↩︎
- Campbell, J., Matoff-Stepp, S., Velez, M. L., Cox, H. H., & Laughon, K. (2021). Pregnancy-Associated Deaths from Homicide, Suicide, and Drug Overdose: Review of Research and the Intersection with Intimate Partner Violence. Journal of Women’s Health (2002), 30(2), 236–244. https://doi.org/10.1089/jwh.2020.8875 ↩︎
- Palladino, C. L., Singh, V., Campbell, J., Flynn, H., & Gold, K. J. (2011). Homicide and suicide during the perinatal period: Findings from the National Violent Death Reporting System. Obstetrics and Gynecology, 118(5), 1056–1063. https://doi.org/10.1097/AOG.0b013e31823294da ↩︎
- Trost, S., Beauregard, J., Chandra, G., Njie, F., Berry, J., Harvey, A., & Goodman, D. A. (2022). Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 36 US States, 2017-2019. ↩︎
- Yu, H., Shen, Q., Bränn, E., Yang, Y., Oberg, A. S., Valdimarsdóttir, U. A., & Lu, D. (2024). Perinatal Depression and Risk of Suicidal Behavior. JAMA Network Open, 7(1), e2350897. https://doi.org/10.1001/jamanetworkopen.2023.50897 ↩︎
- Association of Maternal and Child Health Programs, & Centers for Disease Control and Prevention (CDC). (n.d.). Definitions Used in MMRCs. Review to Action: Working Together To Prevent Maternal Mortality. https://reviewtoaction.org/learn/definitions ↩︎
- Association of Maternal and Child Health Programs, & Centers for Disease Control and Prevention (CDC). (n.d.). Definitions Used in MMRCs. Review to Action: Working Together To Prevent Maternal Mortality. https://reviewtoaction.org/learn/definitions ↩︎
- Wisner, K. L., Sit, D. K. Y., McShea, M. C., Rizzo, D. M., Zoretich, R. A., Hughes, C. L., Eng, H. F., Luther, J. F., Wisniewski, S. R., Costantino, M. L., Confer, A. L., Moses-Kolko, E. L., Famy, C. S., & Hanusa, B. H. (2013). Onset Timing, Thoughts of Self-harm, and Diagnoses in Postpartum Women With Screen-Positive Depression Findings. JAMA Psychiatry, 70(5), 490–498. https://doi.org/10.1001/jamapsychiatry.2013.87 ↩︎
- Spinelli, M. (2021). Postpartum psychosis: A diagnosis for the DSMV. Archives of Women’s Mental Health, 24(5), 817–822. https://doi.org/10.1007/s00737-021-01175-8 ↩︎
- Policy Center for Maternal Mental Health (Director). (2020, October 18). Maternal Suicide: What All Providers and Advocates Should Know [Video recording]. https://www.youtube.com/watch?v=g9J0XbiuCXE ↩︎
- Appleby, L. (1991). Suicide During Pregnancy And In The First Postnatal Year. BMJ: British Medical Journal, 302(6769), 137–140. ↩︎
- Raue, P. J., Ghesquiere, A. R., & Bruce, M. L. (2014). Suicide Risk in Primary Care: Identification and Management in Older Adults. Current Psychiatry Reports, 16(9), 466. https://doi.org/10.1007/s11920-014-0466-8 ↩︎
- Ahmedani, B. K., Simon, G. E., Stewart, C., Beck, A., Waitzfelder, B. E., Rossom, R., Lynch, F., Owen-Smith, A., Hunkeler, E. M., Whiteside, U., Operskalski, B. H., Coffey, M. J., & Solberg, L. I. (2014). Health care contacts in the year before suicide death. Journal of General Internal Medicine, 29(6), 870–877. https://doi.org/10.1007/s11606-014-2767-3 ↩︎
- Ahmedani, B. K., Stewart, C., Simon, G. E., Lynch, F., Lu, C. Y., Waitzfelder, B. E., Solberg, L. I., Owen-Smith, A. A., Beck, A., Copeland, L. A., Hunkeler, E. M., Rossom, R. C., & Williams, K. (2015). Racial/Ethnic differences in health care visits made before suicide attempt across the United States. Medical Care, 53(5), 430–435. https://doi.org/10.1097/MLR.0000000000000335 ↩︎
- Zivin, K., Zhong, C., Rodríguez-Putnam, A., Spring, E., Cai, Q., Miller, A., Johns, L., Kalesnikava, V. A., Courant, A., & Mezuk, B. (2024). Suicide Mortality During the Perinatal Period. JAMA Network Open, 7(6), e2418887. https://doi.org/10.1001/jamanetworkopen.2024.18887 ↩︎
- Reid, H. E., Pratt, D., Edge, D., & Wittkowski, A. (2022). Maternal Suicide Ideation and Behaviour During Pregnancy and the First Postpartum Year: A Systematic Review of Psychological and Psychosocial Risk Factors. Frontiers in Psychiatry, 13. https://www.frontiersin.org/articles/10.3389/fpsyt.2022.765118 ↩︎
- Pigeon, W. R., Pinquart, M., & Conner, K. (2012). Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. The Journal of Clinical Psychiatry, 73(9), e1160-1167. https://doi.org/10.4088/JCP.11r07586 ↩︎
- Sit, D., Luther, J., Buysse, D., Dills, J. L., Eng, H., Okun, M., Wisniewski, S., & Wisner, K. L. (2015). Suicidal ideation in depressed postpartum women: Associations with childhood trauma, sleep disturbance and anxiety. Journal of Psychiatric Research, 66–67, 95–104. https://doi.org/10.1016/j.jpsychires.2015.04.021 ↩︎
- Goldman-Mellor, S., & Margerison, C. E. (2019). Maternal drug-related death and suicide are leading causes of postpartum death in California. American Journal of Obstetrics and Gynecology, 221(5), 489.e1-489.e9. https://doi.org/10.1016/j.ajog.2019.05.045 ↩︎
- Harmer, B., Lee, S., Rizvi, A., & Saadabadi, A. (2024). Suicidal Ideation. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK565877/ ↩︎
- About the Protocol—The Columbia Lighthouse Project. (2016, April 6). https://cssrs.columbia.edu/the-columbia-scale-c-ssrs/about-the-scale/ ↩︎
- Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K. V., Oquendo, M. A., Currier, G. W., Melvin, G. A., Greenhill, L., Shen, S., & Mann, J. J. (2011). The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings From Three Multisite Studies With Adolescents and Adults. The American Journal of Psychiatry, 168(12), 1266–1277. https://doi.org/10.1176/appi.ajp.2011.10111704 ↩︎
- Nilsson, M. E., Suryawanshi, S., Gassmann-Mayer, C., Dubrava, S., McSorley, P., & Jiang, K. (2013). Columbia suicide severity rating scale scoring and Data Analysis Guide. The Columbia Lighthouse Project. https://cssrs.columbia.edu/wp-content/uploads/ScoringandDataAnalysisGuide-for-Clinical-Trials-1.pdf ↩︎
- Trost, S., Beauregard, J., Njie, F., Chandra, G., Berry, J., Goodman, D., & Harvey, A. (2024). Pregnancy-Related Deaths Among American Indian or Alaska Native Persons: Data From Maternal Mortality Review Committees in 36 U.S. States, 2017–2019. Centers for Disease Control and Prevention. https://www.cdc.gov/maternal-mortality/php/data-research/2017-2019-aian.html ↩︎
- Suicide Prevention Resource Center. (2023). SPRC 2023 Tribal Suicide Prevention Needs Assessment: Aggregate Technical Report. https://sprc.org/tna/ ↩︎
- Margerison, C. E., Roberts, M. H., Gemmill, A., & Goldman-Mellor, S. (2022). Pregnancy-Associated Deaths Due to Drugs, Suicide, and Homicide in the United States, 2010-2019. Obstetrics and Gynecology, 139(2), 172–180. https://doi.org/10.1097/AOG.0000000000004649 ↩︎
- Tabb, K., Hsieh, W.-J., Gavin, A., Eigbike, M., Faisal-Cury, A., Mohd Hajaraih, S. K., Huang, W., Laurent, H., Carter, D., Nidey, N., Ryckman, K., & Zivin, K. (2020). Racial differences in immediate postpartum depression and suicidal ideation among women in a Midwestern delivery hospital. Journal of Affective Disorders Reports, 1, 100008. https://doi.org/10.1016/j.jadr.2020.100008 ↩︎
- Policy Center for Maternal Mental Health. (2022, March). Universal Screening for Maternal Mental Health Disorders [Issue Brief]. https://policycentermmh.org/screening-overview/ ↩︎
- Earls, M. F., Yogman, M. W., Mattson, G., Rafferty, J., & COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH. (2019). Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics, 143(1), e20183259. https://doi.org/10.1542/peds.2018-3259 ↩︎
- The American College of Obstetricians and Gynecologists. (2023). Screening and Diagnosis of Mental Health Conditions During Pregnancy and Postpartum. https://www.acog.org/clinical/clinical-guidance/clinical-practice-guideline/articles/2023/06/screening-and-diagnosis-of-mental-health-conditions-during-pregnancy-and-postpartum ↩︎
- Siu, A., & US Preventive Services Task Force. (2016). Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement | Depressive Disorders | JAMA | JAMA Network. https://jamanetwork.com/journals/jama/fullarticle/2484345 ↩︎
- Centers for Medicare & Medicaid Services, V., & Wachino, V. (2016). CMCS Informational Bulletin: Maternal Depression Screening and Treatment: A Critical Role for Medicaid in the Care of Mothers and Children. https://www.medicaid.gov/federal-policy-guidance/downloads/cib051116.pdf ↩︎
- Alliance on Innovation for Maternal Health. (2023). Perinatal Mental Health Conditions. https://saferbirth.org/wp-content/uploads/R1_AIM_Bundle_PMHC.pdf ↩︎
- US Preventive Services Task Force. (2023, June). Depression and suicide risk in adults: Screening. Recommendation: Depression and Suicide Risk in Adults: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/screening-depression-suicide-risk-adults ↩︎
- Zero Suicide. (n.d.). About Zero Suicide. Retrieved August 21, 2024, from https://zerosuicide.edc.org/about ↩︎
- Policy Center for Maternal Mental Health. (n.d.). Maternal Mental Health Screening and Tools. Policy Center for Maternal Mental Health. Retrieved August 21, 2024, from https://policycentermmh.org/screening-overview/ ↩︎
- Suicide Prevention Resource Center. (n.d.). The Patient Safety Screener: A Brief Tool to Detect Suicide Risk. Retrieved August 21, 2024, from https://sprc.org/micro-learning/the-patient-safety-screener-a-brief-tool-to-detect-suicide-risk/ ↩︎
- Zero Suicide. (n.d.). Zero Suicide Toolkit Identify. https://zerosuicide.edc.org/toolkit/identify ↩︎
- Zero Suicide. (n.d.). Zero Suicide Toolkit Engage. https://zerosuicide.edc.org/toolkit/engage ↩︎
- Greydanus, D. E., & Omar, H. A. (2017). Self-cutting and suicide: A review. International Journal of Child Health and Human Development, Suppl. Special Issue: Youth Suicide Prevention, 10(4), 391–396. ↩︎
- Brausch, A. M., & Muehlenkamp, J. J. (2018). Perceived effectiveness of NSSI in achieving functions on severity and suicide risk. Psychiatry Research, 265, 144–150. https://doi.org/10.1016/j.psychres.2018.04.038 ↩︎
- Knorr, A. C., Ammerman, B. A., Hamilton, A. J., & McCloskey, M. S. (2019). Predicting status along the continuum of suicidal thoughts and behavior among those with a history of nonsuicidal self-injury. Psychiatry Research, 273, 514–522. https://doi.org/10.1016/j.psychres.2019.01.067 ↩︎
- Andover, M. S., & Morris, B. W. (2014). Suicidal and nonsuicidal self-injury in the obsessive-compulsive spectrum. In Obsessive-compulsive disorder and its spectrum: A life-span approach. (pp. 241–259). American Psychological Association. https://doi.org/10.1037/14323-013 ↩︎
- Collardeau, F., Corbyn, B., Abramowitz, J., Janssen, P. A., Woody, S., & Fairbrother, N. (2019). Maternal unwanted and intrusive thoughts of infant-related harm, obsessive-compulsive disorder and depression in the perinatal period: Study protocol. BMC Psychiatry, 19(1), 94. https://doi.org/10.1186/s12888-019-2067-x ↩︎
- Abramovitch, A., Abramowitz, J. S., & McKay, D. (2021). The OCI-12: A syndromally valid modification of the obsessive-compulsive inventory-revised. Psychiatry Research, 298, 113808. https://doi.org/10.1016/j.psychres.2021.113808 ↩︎
- Zero Suicide. (n.d.). Zero Suicide Toolkit Evidence. https://zerosuicide.edc.org/toolkit/evidence ↩︎
- Brown, G. K., & Jager-Hyman, S. (2014). Evidence-based psychotherapies for suicide prevention: Future directions. American Journal of Preventive Medicine, 47(3 Suppl 2), S186-194. https://doi.org/10.1016/j.amepre.2014.06.008 ↩︎
- Zero Suicide. (n.d.). Zero Suicide Toolkit Treat. https://zerosuicide.edc.org/toolkit/treat ↩︎
- Brown, G. K., Ten Have, T., Henriques, G. R., Xie, S. X., Hollander, J. E., & Beck, A. T. (2005). Cognitive Therapy for the Prevention of Suicide Attempts: A Randomized Controlled Trial. JAMA, 294(5), 563. https://doi.org/10.1001/jama.294.5.563 ↩︎
- Stanley, B., Brown, G., Brent, D. A., Wells, K., Poling, K., Curry, J., Kennard, B. D., Wagner, A., Cwik, M. F., Klomek, A. B., Goldstein, T., Vitiello, B., Barnett, S., Daniel, S., & Hughes, J. (2009). Cognitive-Behavioral Therapy for Suicide Prevention (CBT-SP): Treatment Model, Feasibility, and Acceptability. Journal of the American Academy of Child & Adolescent Psychiatry, 48(10), 1005–1013. https://doi.org/10.1097/chi.0b013e3181b5dbfe ↩︎
- Eist, H. I. (2015). DBT Skills Training Manual, 2nd Ed. Marsha M. Linehan (2015) New York: The Guilford Press. 504 pp. DBT Skills Training Handouts and Worksheets, 2nd Ed. Marsha M. Linehan (2015) New York: The Guilford Press. 422 pp. Journal of Nervous & Mental Disease, 203(11), 887. https://doi.org/10.1097/nmd.0000000000000387 ↩︎
- Linehan, M. M., Comtois, K. A., Murray, A. M., Brown, M. Z., Gallop, R. J., Heard, H. L., Korslund, K. E., Tutek, D. A., Reynolds, S. K., & Lindenboim, N. (2006). Two-Year Randomized Controlled Trial and Follow-up of Dialectical Behavior Therapy vs Therapy by Experts for Suicidal Behaviors and Borderline Personality Disorder. Archives of General Psychiatry, 63(7), 757. https://doi.org/10.1001/archpsyc.63.7.757 ↩︎
- Ryberg, W., Zahl, P.-H., Diep, L. M., Landrø, N. I., & Fosse, R. (2019). Managing suicidality within specialized care: A randomized controlled trial. Journal of Affective Disorders, 249, 112–120. https://doi.org/10.1016/j.jad.2019.02.022 ↩︎
- Andreasson, K., Krogh, J., Wenneberg, C., Jessen, H. K. L., Krakauer, K., Gluud, C., Thomsen, R. R., Randers, L., & Nordentoft, M. (2016). EFFECTIVENESS OF DIALECTICAL BEHAVIOR THERAPY VERSUS COLLABORATIVE ASSESSMENT AND MANAGEMENT OF SUICIDALITY TREATMENT FOR REDUCTION OF SELF-HARM IN ADULTS WITH BORDERLINE PERSONALITY TRAITS AND DISORDER-A RANDOMIZED OBSERVER-BLINDED CLINICAL TRIAL: Research Article: Effectiveness of DBT versus CAMS on Reducing Self-Harm. Depression and Anxiety, 33(6), 520–530. https://doi.org/10.1002/da.22472 ↩︎
- Swift, J. K., Trusty, W. T., & Penix, E. A. (2021). The effectiveness of the Collaborative Assessment and Management of Suicidality (CAMS) compared to alternative treatment conditions: A meta‐analysis. Suicide and Life-Threatening Behavior, 51(5), 882–896. https://doi.org/10.1111/sltb.12765 ↩︎
- Jobes, D. A., Comtois, K. A., Gutierrez, P. M., Brenner, L. A., Huh, D., Chalker, S. A., Ruhe, G., Kerbrat, A. H., Atkins, D. C., Jennings, K., Crumlish, J., Corona, C. D., Connor, S. O., Hendricks, K. E., Schembari, B., Singer, B., & Crow, B. (2017). A Randomized Controlled Trial of the Collaborative Assessment and Management of Suicidality versus Enhanced Care as Usual With Suicidal Soldiers. Psychiatry, 80(4), 339–356. https://doi.org/10.1080/00332747.2017.1354607 ↩︎
- Jobes, D. A., Wong, S. A., Conrad, A. K., Drozd, J. F., & Neal‐Walden, T. (2005). The Collaborative Assessment and Management of Suicidality versus Treatment as Usual: A Retrospective Study with Suicidal Outpatients. Suicide and Life-Threatening Behavior, 35(5), 483–497. https://doi.org/10.1521/suli.2005.35.5.483 ↩︎
- Ahmedani, B. K., & Vannoy, S. (2014). National Pathways for Suicide Prevention and Health Services Research. American Journal of Preventive Medicine, 47(3), S222–S228. https://doi.org/10.1016/j.amepre.2014.05.038 ↩︎
- Substance Abuse and Mental Health Services Administration. (2014, April 3). Screening, Brief Intervention, and Referral to Treatment (SBIRT). https://www.samhsa.gov/sbirt ↩︎
- Stanley-Brown Safety Planning Intervention. (n.d.). Stanley-Brown Safety Planning Intervention. Retrieved August 21, 2024, from https://suicidesafetyplan.com/ ↩︎
- Stanley, B., & Brown, G. K. (2012). Safety Planning Intervention: A Brief Intervention to Mitigate Suicide Risk. Cognitive and Behavioral Practice, 19(2), 256–264. https://doi.org/10.1016/j.cbpra.2011.01.001 ↩︎
- Substance Abuse and Mental Health Services Administration. (2014, June). Crisis Services: Effectiveness, Cost-Effectiveness, and Funding Strategies. https://store.samhsa.gov/product/crisis-services-effectiveness-cost-effectiveness-and-funding-strategies/sma14-4848 ↩︎
- Policy Center for Maternal Mental Health. (n.d.). Maternal Mental Health Peer Support. Policy Center for Maternal Mental Health – Formerly 2020 Mom. Retrieved August 25, 2024, from https://policycentermmh.org/certified-peer-support/ ↩︎
- Centers for Medicare & Medicaid Services. (n.d.). Partial Hospitalization Coverage. Retrieved August 25, 2024, from https://www.medicare.gov/coverage/mental-health-care-partial-hospitalization ↩︎
- Postpartum Support International (PSI). (n.d.). Intensive Treatment in the US. Retrieved August 25, 2024, from https://www.postpartum.net/get-help/intensive-perinatal-psych-treatment-in-the-us/ ↩︎
- Jobes, D. A. (2012). The Collaborative Assessment and Management of Suicidality (CAMS): An Evolving Evidence‐Based Clinical Approach to Suicidal Risk. Suicide and Life-Threatening Behavior, 42(6), 640–653. https://doi.org/10.1111/j.1943-278x.2012.00119.x ↩︎
- Bickley, H., Hunt, I. M., Windfuhr, K., Shaw, J., Appleby, L., & Kapur, N. (2013). Suicide Within Two Weeks of Discharge From Psychiatric Inpatient Care: A Case-Control Study. Psychiatric Services, 64(7), 653–659. https://doi.org/10.1176/appi.ps.201200026 ↩︎
- Office of the Surgeon General (US), & National Action Alliance for Suicide Prevention (US). (2012). 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action: A Report of the U.S. Surgeon General and of the National Action Alliance for Suicide Prevention. US Department of Health & Human Services (US). https://www.ncbi.nlm.nih.gov/books/NBK109906/ ↩︎
- Carr, C. (2018, May). Recommended Standard Care for People with Suicide Risk: A Critical Step Forward – Suicide Prevention Resource Center. https://sprc.org/news/recommended-standard-care-for-people-with-suicide-risk-a-critical-step-forward/ ↩︎
- Layman, D. M., Kammer, J., Leckman-Westin, E., Hogan, M., Goldstein Grumet, J., Labouliere, C. D., Stanley, B., Carruthers, J., & Finnerty, M. (2021). The Relationship Between Suicidal Behaviors and Zero Suicide Organizational Best Practices in Outpatient Mental Health Clinics. Psychiatric Services, 72(10), 1118–1125. https://doi.org/10.1176/appi.ps.202000525 ↩︎
- U.S. Department of Health and Human Services (HHS). (2024, April 15). 2024 National Strategy for Suicide Prevention [Text]. https://www.hhs.gov/programs/prevention-and-wellness/mental-health-substance-abuse/national-strategy-suicide-prevention/index.html ↩︎
- Chin, K., Wendt, A., Bennett, I. M., & Bhat, A. (2022). Suicide and Maternal Mortality. Current Psychiatry Reports, 24(4), 239–275. https://doi.org/10.1007/s11920-022-01334-3 ↩︎
- Burkhard, J. (2018, September 10). Maternal Suicide Tracking in the U.S. – We’re Getting Closer. Retrieved from. Policy Center for Maternal Mental Health. https://policycentermmh.org/maternal-suicide-tracking-in-the-u-s-were-getting-closer/ ↩︎
- Smid, M. C., Maeda, J., Stone, N. M., Sylvester, H., Baksh, L., Debbink, M. P., Varner, M. W., & Metz, T. D. (2020). Standardized Criteria for Review of Perinatal Suicides and Accidental Drug-Related Deaths. Obstetrics & Gynecology, 136(4), 645–653. https://doi.org/10.1097/aog.0000000000003988 ↩︎
- Centers for Disease Control and Prevention (CDC). (2024, August). Enhancing Reviews and Surveillance to Eliminate Maternal Mortality. Maternal Mortality Prevention. https://www.cdc.gov/maternal-mortality/php/erase-mm/index.html ↩︎
- Centers for Disease Control and Prevention (CDC). (2024, August 27). Biden-Harris Administration Awards Over $558 Million to Improve Maternal Health, including $440 Million to Support Pregnant and New Moms, Infants, and Children through Voluntary Home Visiting Programs Proven to Improve Maternal and Child Health, Child Development, and School Readiness. CDC Newsroom. https://www.cdc.gov/media/releases/2024/p0827-maternal-health.html ↩︎
- Centers for Disease Control and Prevention (CDC). (2019). Informant Interview Guide for Maternal Mortality Review Committees. https://www.cdc.gov/maternal-mortality/media/pdfs/MMRC-Informant-Interview-Guide_tagged_508c.pdf ↩︎
- Centers for Disease Control and Prevention (CDC). (2024, May 20). State Perinatal Quality Collaboratives. Maternal Infant Health. https://www.cdc.gov/maternal-infant-health/pqc/state-pqcs.html ↩︎
- Trost, S. L., Beauregard, J. L., Smoots, A. N., Ko, J. Y., Haight, S. C., Moore Simas, T. A., Byatt, N., Madni, S. A., & Goodman, D. (2021). Preventing Pregnancy-Related Mental Health Deaths: Insights From 14 US Maternal Mortality Review Committees, 2008–17: Health Affairs, 40(10), 1551–1559. https://doi.org/10.1377/hlthaff.2021.00615 ↩︎
- Lynch, F. L., Peterson, E. L., Lu, C. Y., Hu, Y., Rossom, R. C., Waitzfelder, B. E., Owen-Smith, A. A., Hubley, S., Prabhakar, D., Keoki Williams, L., Beck, A., Simon, G. E., & Ahmedani, B. K. (2020). Substance use disorders and risk of suicide in a general US population: A case control study. Addiction Science & Clinical Practice, 15(1), 14. https://doi.org/10.1186/s13722-020-0181-1 ↩︎
- National Institutes on Drug Abuse (US). (2020). Common Comorbidities with Substance Use Disorders Research Report. http://www.ncbi.nlm.nih.gov/books/NBK571451/ ↩︎
- Centers for Disease Control and Prevention (CDC). (2024, August 9). Suicide Prevention. Suicide Prevention. https://www.cdc.gov/suicide/index.html ↩︎
- Admon, L. K., Dalton, V. K., Kolenic, G. E., Ettner, S. L., Tilea, A., Haffajee, R. L., Brownlee, R. M., Zochowski, M. K., Tabb, K. M., Muzik, M., & Zivin, K. (2021). Trends in Suicidality 1 Year Before and After Birth Among Commercially Insured Childbearing Individuals in the United States, 2006-2017. JAMA Psychiatry, 78(2), 171–176. https://doi.org/10.1001/jamapsychiatry.2020.3550 ↩︎
- Zero Suicide. (n.d.). Zero Suicide Toolkit Train. https://zerosuicide.edc.org/toolkit/train ↩︎
- Richtel, M. (2022, August 27). The Best Tool We Have’ for Self-Harming and Suicidal Teens. The New York Times. https://www.nytimes.com/2022/08/27/health/dbt-teens-suicide.html ↩︎
- Policy Center for Maternal Mental Health. (2020, November 20). The National Zero Suicide Initiative Levers for Maternal Mental Health. https://www.youtube.com/watch?v=wr-_8vCrquw ↩︎


