On July 25th, 2023, the Departments of Labor, Health and Human Services and the Treasury announced proposed rules to strengthen the Mental Health Parity and Addiction Equity Act. We have been honored to be a part of shaping these rules with the Department of Labor and The Kennedy Forum over the past several years. This week the Policy Center for Maternal Mental Health submitted the following letter in response to the proposed rules.
Our work shaping and reporting on national mental health policy is made possible through a 2020-2023 capacity grant from the Perigee Fund.
RE: Requirements Related to the Mental Health Parity and Addiction Equity Act (MHPAEA)
Dear Secretary Becerra, Assistant Secretary Gomez, and Deputy Commissioner O’Donnell,
The Policy Center for Maternal Mental Health is a national nonprofit whose mission is to close gaps in maternal mental healthcare. One of our primary focus areas is addressing gaps in insurance coverage and access. We appreciate the opportunity to comment on the Department of Health and Human Services (HHS), Employee Benefits Security Administration (DOL-EBSA)and the Internal Revenue Service’s (the “Departments”) proposed rule, Requirements Related to the Mental Health Parity and Addiction Equity Act (hereinafter ”Proposed Rule”).
We strongly support the Proposed Rule’s aim to increase access by ensuring behavioral health insurers’ treatment limitations are no more restrictive than medical surgical insurers’ limits.
We appreciate the reference to maternal mental health in the Proposed Rule, explaining, “By increasing access to services, these proposed rules would lead to more people receiving treatment, reducing the burden on family members and other support systems. This includes untreated maternal mental health conditions (MMHCs), which can lead to a reduced ability to work, increased risk of suicide, increased use of public services such as Medicaid, and worse maternal and child health.”
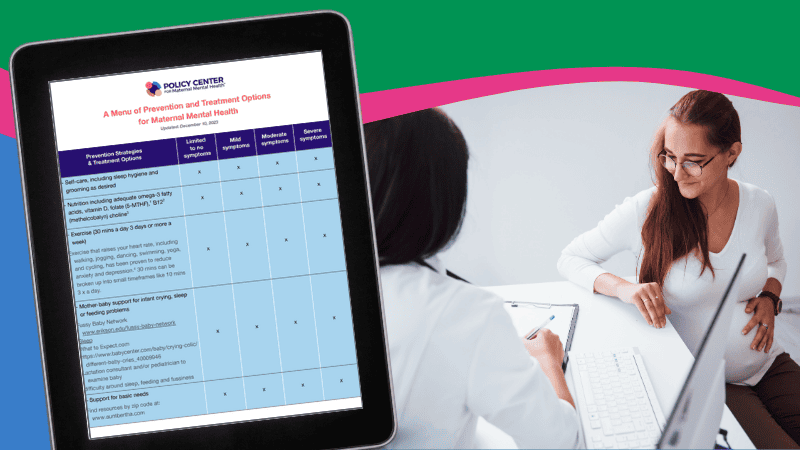
In addition, we appreciate the DOL citing the economic impact of untreated MMHDs. Several states have conducted their own analysis, including Texas:
“A 2022 study of the cost of MMHC to Texas women and their children projected costs for the 2019 birth cohort from the time of conception through five years postpartum to total $2.2 billion. Untreated MMHCs include untreated perinatal mood and anxiety disorders (PMADs), which have been found to account for approximately $48 million in societal costs in Vermont for the average annual birth cohort from conception through five years postpartum, including $12.5 million in productivity loss and $9.4 million in non-obstetric health expenditures. The cost in missed productivity due to workers’ fair or poor mental health was estimated as $47.6 billion annually in 2022. A 2022 study found that households with a family member diagnosed with a mental health disorder had lower health status scores compared to households without a mental illness diagnosis, suggesting evidence of family spillover effects on mental illness.”
The maternal population should be treated as a specialized population, and plans should specifically be required to monitor access and MHPAEA compliance.
We are pleased with the statement of purpose noting plans to analyze the impact of nonquantitative treatment limitations (NQTLs) on access to MH/SUD services as part of the comparative analysis requirement.
We further support the data collection and reporting requirements, especially with respect to the comparative analyses of NQTLs and network composition, and request that network adequacy requirements include subspecialty assessment. For example, a plan shouldn’t just assess the number of LCSWs and MDs but rather the provider’s subspecialty as medical networks are assessed for subspecialty (dermatology, cardiology, etc.). In the case of maternal mental health, the subspecialty “Perinatal Mental Health-Certified” should be assessed for network adequacy. Additionally, plans should be required to state how they are covering certified peer support specialists (CPSSs). For example, are CPSSs billed under any licensed behavioral health provider’s National Provider Identifier? This should be explained. Additionally, it should be clear how members/patients can find which behavioral health providers are certified peers in provider directories.
Further, we believe plans should be offering access to psychiatrists for PCP/obstetric provider consultation for both general psychiatry and psychiatry with an emphasis on maternal mental health. This should be made clear in plan materials, and access should be monitored with quality improvement plans in place until access to consultations reaches expected levels based on the plan’s population.
We strongly support the Departments anchoring MHPAEA, including its implementing regulations, to determine whether plans/issuers’ treatment limitations disparately limit access to MH/SUD treatment.
In addition, as suggested by the Kennedy Forum, we urge the Department to make an important technical correction in the next-to-last sentence in (a)(1), which states: “… then they impose on access to generally comparable medical/surgical benefits.” This language should be revised to state, “… then they impose on access to medical/surgical benefits in the same benefit classification group.” Evaluation of plans/issuers’ MHPAEA compliance is always bounded by the relevant benefit classification group. Introduction of the phrase “generally comparable medical/surgical benefits” in (a)(1) to describe types of benefits under a plan could lead to uncertainty and confusion because the term “comparable” used in the current rule and the offered examples to describe only the limitations placed upon benefits – not to compare the benefits themselves. Additionally, attempting to identify “generally
comparable” MH/SUD and M/S benefits (other than through benefit classification groups) is fraught with difficulty, which is why it has previously been rejected. We urge the Departments to remove the words “generally comparable” in this instance in order to clarify that the “benefit classification group” will continue to how MHPAEA compliance is evaluated.
Further, in the section “Substantially All / Predominant Test for NQTLs – (c)(4)(i),” we urge the Departments to require plans to document in their NQTL analysis how their clinical standards and practices deviate from independent professional medical or clinical standards using a definition “independent professional medical or clinical standards.” This includes drugs
approved by the United States Food and Drug Administration, recommendations of nonprofit healthcare provider professional associations/societies (including medical societies), and level of care and clinical practice guidelines. Guidelines have recently been published by the American College of Obstetrics and Gynecology.
Additionally, should a plan/issuer deny authorization for a specific level of care, the plan/issuer must identify a lower level of care that it believes would be more appropriate, along with information related to the coverage of such service in the plan and the availability of network providers to deliver the lower level of service.
We urge the Departments to clarify that outcome data must be separately reported for
MH and SUD services to conform to the statutory standard and that subspecialities be further reported. Specifically, our interest is in seeing maternal mental health data reported separately/disaggregated from other mental health data. We urge the Departments to require plans to take action whenever the data shows any difference in access.
Finally, we strongly support the language implementing the elimination of self-funded non-federal governmental plans’ ability to opt out of MHPAEA. Hundreds of thousands of public
employees and their family members have for too long been denied critical MHPAEA protections. Self-funded plan sponsors and Third Party Administrators (TPAs) should be accountable for MHPAEA compliance, given their direct role in processing claims, maintaining provider networks, and conducting utilization reviews.
We strongly urge the Departments to adopt maximum appointment wait time standards in addition to network adequacy standards. The Departments should ensure that participants/beneficiaries who cannot access in-network services on a timely basis can access out-of-network services, with their out-of-pocket costs no greater than the amounts that they would have paid for the same services received from an in-network provider.
Thank you for the opportunity to comment on this important issue. If you have further questions, please contact Sarah Johanek at [email protected].
Sincerely,
Joy Burkhard, MBA
Executive Director
[email protected]